On November 13, 2025, the US Food and Drug Administration approved pertuzumab-dpzb (Poherdy) as an interchangeable biosimilar to pertuzumab (Perjeta) for the treatment of HER2-positive breast cancer, consistent with the indications of the reference product.
The approval was based on analytical, nonclinical, and clinical data establishing biosimilarity and interchangeability with the reference product. Evidence included a pharmacokinetic study and a comparative clinical trial in patients with HER2-positive breast cancer, demonstrating no clinically meaningful differences in safety, purity, or potency.
No new safety signals were observed. The safety profile of pertuzumab-dpzb is expected to reflect that of pertuzumab, with common adverse reactions including diarrhea, alopecia, neutropenia, nausea, fatigue, rash, and peripheral neuropathy. Serious risks include left ventricular dysfunction and infusion-related reactions.
Pertuzumab-dpzb is the first interchangeable biosimilar to pertuzumab approved in the United States. The interchangeable designation permits pharmacy-level substitution, where state law allows, and may increase access while reducing treatment costs for patients with HER2-positive breast cancer.
Reference US Food and Drug Administration. FDA approves new interchangeable biosimilar to Perjeta. Published November 13, 2025. Accessed November 18, 2025. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-new-interchangeable-biosimilar-perjeta
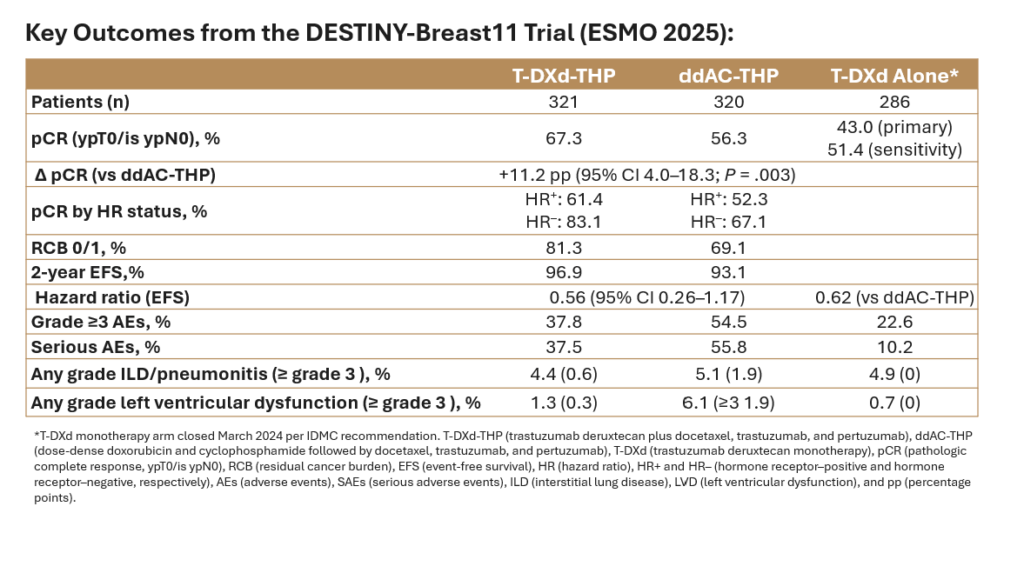
At the 2025 European Society for Medical Oncology (ESMO) Congress, Nadia Harbeck, MD, of the University of Munich, presented results of the phase 3 DESTINY-Breast11 trial, marking the first randomized evidence that an antibody–drug conjugate–based neoadjuvant regimen can outperform anthracycline-containing chemotherapy in human epidermal growth factor receptor 2 (HER2)-positive early breast cancer (eBC).
The global, open-label phase 3 study randomized 927 patients with HER2-positive eBC to receive (1:1:1) trastuzumab deruxtecan plus docetaxel, trastuzumab, and pertuzumab (T-DXd-THP), dose-dense doxorubicin and cyclophosphamide followed by docetaxel, trastuzumab, and pertuzumab (ddAC-THP), or trastuzumab deruxtecan monotherapy (T-DXd). The primary endpoint of the study was pathologic complete response (pCR) by blinded central review, and key secondary endpoints included event-free survival (EFS), invasive disease-free survival (iDFS), overall survival (OS), and safety.
Median patient age was 50 years, 73% were hormone receptor (HR)–positive, and 89% had node-positive disease.
The trial met its primary endpoint with T-DXd-THP achieving a pCR rate of 67.3% compared with 56.3% with ddAC-THP, an absolute difference of 11.2 percentage points (95% CI 4.0–18.3; P = .003). The benefit was observed in both HR-positive and HR-negative groups and independent of menopausal or HER2 status (IHC3+ vs other) status.
Residual cancer burden (RCB) analyses echoed this finding: 81.3% of patients on T-DXd-THP had RCB 0/1, compared with 69.1% in the control arm.
Event-free survival data were immature at the time of analysis but trended in favor of T-DXd-THP (HR, 0.56; 95% CI, 0.26–1.17). T-DXd monotherapy showed inferior EFS compared to ddAC-THP and was closed on March 13, 2024, as recommended by the independent data monitoring committee.
Treatment with T-DXd-containing regimens resulted in fewer grade 3 or higher adverse events (AEs), lower hematologic toxicity, fewer treatment interruptions, and less left-ventricular dysfunction. The incidence of interstitial lung disease (ILD) was comparable between arms. T-DXd-THP treatment resulted in higher rates of nausea but were similar for other gastrointestinal toxicities. Adverse events leading to surgical delay occurred in 3.4% of T-DXd-THP patients vs 2.6% of those receiving ddAC-THP.
Overall, the DESTINY-Breast11study showed that the combination of T-DXd with THP resulted in the highest pCR rates for a registrational trial to date with lower toxicity for patients with HER2+ eBC and may redefine the neoadjuvant standard for high-risk HER2-positive eBC, but longer-term outcomes are awaited. The study was published simultaneously to presentation in the Annals of Oncology.
References
Harbeck N, et al. Trastuzumab deruxtecan–based neoadjuvant therapy in high-risk HER2-positive early breast cancer. Abstract 291O, presented at: ESMO 2025 Congress; October 2025; Barcelona, Spain.
Harbeck N, Modi S, Pusztai L, et al. Neoadjuvant trastuzumab deruxtecan alone or followed by paclitaxel, trastuzumab, and pertuzumab for high-risk HER2-positive early breast cancer (DESTINY-Breast11): a randomised, open-label, multicentre, phase 3 trial.