WU-KONG28
ASCO 2026
Sunvozertinib vs platinum-based chemotherapy · First-line advanced NSCLC with EGFR exon20ins · International randomized phase 3
Total N
324
1:1 randomized
Median PFS
10.3 vs 7.5 mo
Sunvo vs Chemo
Hazard Ratio
0.65
95% CI 0.50–0.85 · P<0.001
Confirmed ORR
58.9% vs 31.1%
Sunvo vs Chemo
WU-KONG28 Study Design
Key Eligibility
- Locally advanced or metastatic non-squamous NSCLC
- Documented EGFR exon20ins
- Newly diagnosed or treatment-naïve
- ECOG PS 0 or 1
Randomization
Ratio1:1
StratificationBaseline brain metastasis (yes / no)
Sites154 sites · 15 countries
Data cutoffJanuary 16, 2026
Sunvozertinib (N=163)
300 mg once daily, oral
Continuous until progression or unacceptable toxicity
Continuous until progression or unacceptable toxicity
Platinum-based Chemotherapy (N=161)
Carboplatin AUC5 + pemetrexed 500 mg/m² Q3W
Up to 4 or 6 cycles (investigator discretion) → pemetrexed maintenance
Crossover to sunvozertinib allowed at confirmed PD
Up to 4 or 6 cycles (investigator discretion) → pemetrexed maintenance
Crossover to sunvozertinib allowed at confirmed PD
Endpoints
Primary
PFS assessed by BICR
Key Secondary
Overall Survival (OS)
Secondary
Investigator-assessed PFS · ORR · DCR · DoR · Tumor size change · Safety · PK
Exploratory
PFS2
Efficacy
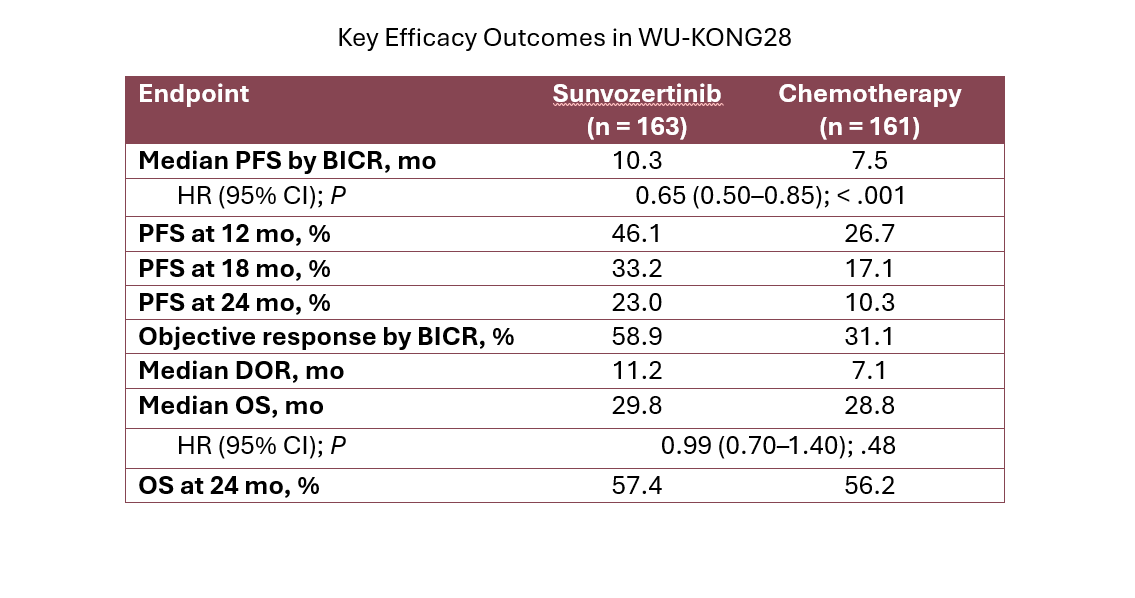
Primary Endpoint: Median PFS (BICR)
HR (95% CI)0.65 (0.50, 0.85)
P value<0.001
PFS Landmark Rates
12 months46.1% vs 26.7%
18 months33.2% vs 17.1%
24 months23.0% vs 10.3%
Median follow-up: 24.0 mo (sunvo) · 18.0 mo (chemo)
Objective Response Rate (BICR)
Confirmed ORR
Odds Ratio (95% CI)3.2 (2.0, 5.0)
Additional Response Data (from ASCO presentation)
Best ORR68.1% vs 35.4%
Disease Control Rate94.5% vs 85.7%
Duration of Response
Median follow-up: 22.1 mo (sunvo) · 13.8 mo (chemo)
Median Tumor Size Shrinkage
Crossover
101 of 112 chemotherapy-arm patients (90.2%) with confirmed disease progression crossed over to receive sunvozertinib.
Interim Overall Survival
HR (95% CI)0.99 (0.70, 1.40)
P value0.48
Data maturity38.9% (126/324 events)
OS Landmark Rates
18 months65.5% vs 67.2%
24 months57.4% vs 56.2%
30 months50.0% vs 49.1%
Median OS follow-up: 26.1 mo (sunvo) · 26.7 mo (chemo). OS data immature; interpretation may be confounded by the crossover design. NE, not estimable.
Subgroup Analysis: BICR-assessed PFS
← Favors sunvozertinib
HR = 1.0
Favors chemotherapy →
Overall(n=324)
0.65 (0.50, 0.85)
Age Group
<65 years(n=182)
0.62 (0.44, 0.87)
≥65 years(n=142)
0.71 (0.46, 1.07)
Sex
Female(n=192)
0.68 (0.48, 0.97)
Male(n=132)
0.58 (0.39, 0.85)
Race
Asian(n=204)
0.56 (0.41, 0.77)
Non-Asian(n=120)
0.93 (0.58, 1.48)
Region
North America + EU(n=102)
0.78 (0.47, 1.30)
Others(n=222)
0.62 (0.45, 0.84)
Smoking History
Never(n=208)
0.61 (0.43, 0.85)
Ever(n=116)
0.73 (0.48, 1.11)
Baseline ECOG
0(n=89)
0.77 (0.45, 1.31)
≥1(n=235)
0.62 (0.46, 0.84)
Brain Metastasis at Baseline
With(n=41)
0.96 (0.44, 2.08)
Without(n=283)
0.62 (0.47, 0.83)
EGFR Exon20ins Subtype
769_ASV(n=103)
0.46 (0.29, 0.73)
770_SVD(n=53)
NR
Other/Unknown(n=168)
0.77 (0.53, 1.10)
EGFR Exon20ins Region
Near loop(n=220)
0.59 (0.43, 0.82)
Far loop(n=84)
0.83 (0.49, 1.38)
C-helix/Unknown(n=20)
NR
Disease-Related Surgery
With(n=65)
0.55 (0.29, 1.02)
Without(n=259)
0.69 (0.51, 0.92)
X-axis range: 0.2 to 2.5. NR = not reported (insufficient events). Source: Heymach et al, ASCO 2026 LBA8500 (slide 7).
Safety
Sunvozertinib N=163; Chemotherapy N=150 (patients who received randomized treatment)
Safety Overview
| Parameter | Sunvozertinib % | Chemotherapy % |
|---|---|---|
| Any adverse event | 100.0 | 99.3 |
| Any AE, Grade ≥3 | 75.5 | 56.7 |
| Any TRAE | 100.0 | 97.3 |
| Any TRAE, Grade ≥3 | 61.3 | 49.3 |
| Treatment-related SAE | 18.4 | 12.7 |
| TRAE leading to dose interruption | 45.4 | 27.3 |
| TRAE leading to dose reduction | 40.5 | 24.0 |
| TRAE leading to discontinuation | 7.4 | 11.3 |
| TRAE with fatal outcome | 0.0 | 0.7 |
Top TRAEs leading to dose interruption and reduction with sunvozertinib: CPK increased and diarrhea (neither led to treatment discontinuation).
Adverse Events ≥20% in Either Group (Any Grade)
All-cause adverse events emerging during treatment (per NEJM Table 3). Grade ≥3 shown in adjacent column.
Sunvo
G≥3
Chemo
G≥3
Diarrhea
14.1%
—
CPK increased
20.9%
0.7%
Anemia
9.2%
11.3%
Rash
0.6%
—
Paronychia
3.7%
—
Weight decreased
3.7%
0.7%
Decreased appetite
1.8%
1.3%
Creatinine increased
0.6%
—
Nausea
1.8%
1.3%
Vomiting
1.8%
2.0%
Hypokalemia
3.7%
0.7%
Amylase increased
1.2%
—
Lipase increased
5.5%
1.3%
AST increased
2.5%
0.7%
Mouth ulceration
1.2%
—
ALT increased
1.8%
1.3%
Fatigue
1.2%
2.7%
Neutrophil ↓
2.5%
18.7%
WBC ↓
0.6%
6.7%
Constipation
0.6%
—
Platelet ↓
2.5%
6.7%
Sunvozertinib AEs reflect wild-type EGFR inhibition (diarrhea, rash, paronychia, CPK elevation). Chemotherapy-associated myelosuppression (anemia, neutropenia, thrombocytopenia) predominates in the chemo arm.
References
- Heymach JV, Liu G, Xing L, et al. Sunvozertinib monotherapy versus platinum-based chemotherapy as first-line treatment for advanced NSCLC with EGFR exon20ins: primary analysis of a multinational phase 3 randomized study (WU-KONG28). J Clin Oncol. 2026;44(suppl 17):LBA8500. doi:10.1200/JCO.2026.44.17_suppl.LBA8500. Presented at: 2026 ASCO Annual Meeting; May 29–June 2, 2026; Chicago, IL.
- Zhou C, Greillier L, Liu G, et al. First-line sunvozertinib in NSCLC with EGFR exon 20 insertion mutations. N Engl J Med. 2026. doi:10.1056/NEJMoa2604461.
- ClinicalTrials.gov identifier: NCT05668988.
Abbreviations
BICRBlinded Independent Central Review
cORRConfirmed Objective Response Rate
CPKCreatine phosphokinase
DCRDisease Control Rate
DoRDuration of Response
ECOGEastern Cooperative Oncology Group
EGFREpidermal Growth Factor Receptor
Exon20insExon 20 Insertion Mutations
HRHazard Ratio
mPFSMedian Progression-Free Survival
NSCLCNon-Small Cell Lung Cancer
ORRObjective Response Rate
OSOverall Survival
PFSProgression-Free Survival
PFS2Second Progression-Free Survival
Q3WEvery 3 Weeks
SAESerious Adverse Event
TKITyrosine Kinase Inhibitor
TRAETreatment-Related Adverse Event